 Dr. B.K. Rao
Dr. B.K. Rao
 Dr. Prakash Shastri
Dr. Prakash Shastri
 Dr. Vinod Kumar Singh
Dr. Vinod Kumar Singh
 Dr. Debashis Dhar
Dr. Debashis Dhar
 Dr. S.C. Sharma
Dr. S.C. Sharma
 Dr. Ashok Anand
Dr. Ashok Anand
 Dr. Sanjeev Mittal
Dr. Sanjeev Mittal
 Dr. Ashutosh Taneja
Dr. Ashutosh Taneja
 Dr. Niraj Tyagi
Dr. Niraj Tyagi
 Dr. Saurabh Taneja
Dr. Saurabh Taneja
 Dr. Prasoon Gupta
Dr. Prasoon Gupta
 Dr. Rahul Kumar
Dr. Rahul Kumar
 Dr. Asish Kr. Sahoo
Dr. Asish Kr. Sahoo
Critical Care Medicine (CCM) is a specialty that involves the management of patients with life threatening, frequently complex medical and surgical illnesses in a specialized Intensive Care Unit (ICU) or similar facility. A modern ICU represents the pinnacle of any hospital’s approach to highly technological & sophisticated in-patient care. The CCM physician, also called an Intensivist in some parts of the world, has expertise in the evaluation and management of these critically ill patients.
These critically ill patients may have dysfunction or failure of one or more organ systems, including the cardiac, pulmonary, neurologic, liver, kidney or gastrointestinal systems. In the ICU procedures used to support and identify the cause of the critical illness include endotracheal intubation, central venous catheterization, arterial cannulation, pulmonary artery catheterization, bronchoscopy, lumbar puncture, thoracocentesis, paracentesis, chest tube thoracostomy and percutaneous tracheostomy. Specialists from anaesthesia, general medicine, pulmonology and surgery can undergo further training in critical care medicine to become a CCM physician.
The Instt. of Critical Care Medicine at Sir Ganga Ram Hospital is recognized both nationally and internationally as a leader in patient care, research and training. Today the Instt. of Critical Care Medicine is amongst the largest in private hospitals. The department has 80 critical care beds including 12 beds in the Executive block. The department also provides resuscitation and critical care services to High Dependency Units (HDU), floor beds and Emergency department.The Instt. of Critical Care Medicine at Sir Ganga Ram Hospital is recognized both nationally and internationally as a leader in patient care, research and training. Today the Instt. of Critical Care Medicine is amongst the largest in private hospitals. The department has 80 critical care beds including 12 beds in the Executive block. The department also provides resuscitation and critical care services to High Dependency Units (HDU), floor beds and Emergency department. All beds are equipped with GE Multichannel physiological monitoring systems allowing close monitoring of patients both from the bedside and the central nursing station. The patient beds are totally motorized for enhanced patient comfort and care. Organ support systems like ventilators including High Frequency Oscillatory Ventilator and Nitric Oxide delivery system; Conventional ve ntilators with latest ventilatory modes and respiratory mechanics analysis facilities, Hemodialysis and CRRT machines; ECMO and MARS machine are available at the bedside. Flexible Fiberoptic Bronchosco py, Ultrasonography and Echocardiography are housed in the ICU and are used routinely for both diagnostic and therapeutic purpose.
Patients from across the country are transported via ground and air ambulance services which are fully equipped with life support systems, ventilators and monitors; a trained doctor and technician accompanies the patient during transportation.
A regular teaching schedule in the form of seminars, case presentations and journal discussions is held for the 24 trainee fellows (NBE: 3-year and ISCCM: 1-year course). Few candidates on short 3 or 6 month observation courses are provided introductory critical care orientation.
Quarterly Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS) training (American Heart Association certified) is conducted in hospital premises. Monthly data collection and yearly audit is performed as aquality improvementprocess that seeks to improve patient care and outcomes through systematic review of care against established global benchmarks.
ECMO Programme :
Programme Director: Dr. B.K. Rao
Co-Director: Dr. Vinod K. Singh
Programme Coordinator: Dr. Sanjeev Mittal
The Department started offering ECMO to suitable patients in 2014
The team associated with the Extra Corporeal Membrane Oxygenation (ECMO) program has the experience of carrying out both forms of ECMO, Veno Arterial(VA) and Veno Venous(VV).
The indications for both types are different and depend on the target organ support.
Till now, the team has done over 20 cases of both modalities and is well versed with the intricacies of both.
We regularly share our data with Extracorporeal Life Support Organization (ELSO), the umbrella organization for ECMO worldwide. The data sharing is both ways between ELSO and our institute as a part of the academic programme.
We conduct regular training programmes in ECMO.
Our Team members are Part of committee of ECMO society of India and we are in process of launching a fellowship program in ECMO under the aegis of ECMO Society of India
Our ECMO success rates have been comparable to international centers, both for VA and VV ECMO.
We take pride in offering highest quality ECMO treatment at affordable cost.
With continued improvement in skills and training at international centers, the team aspires to further improve upon its successes.
International Training Center of American Heart Association:
Sir Ganga Ram Hospital was earlier training Layman and medical professionals in Basic Life and Advanced Cardiac life Support Provider program as a satellite center of American Heart association through St Johns Medical College and Manipal Hospital Bangalore.
Since we already had a good infrastructure and a highly experienced set of instructors we have signed an agreement with AHA and are now recognized as an Independent ITC of AHA for all adult training Programs.
We take pride in training over a thousand of Medical professionals in last ten years as BLS and ACLS providers.
We continue to emphasize highest training and educational standards within the parameters of AHA.
We conduct all adult training courses including Instructor Courses.
The training is conducted at a very affordable fee structure (on a cost only basis).
Important Milestones:
Annual Conference-cum-Workshop
The department conducts an annual academic festival inviting delegates and faculty from all over the country from the year 2013. The theme focuses on the latest practices in the field of critical care every year.
Consultants and Staff:
Current DNB Fellows:
2021-2024:
2022-2025:
2023-2026:
Current IDCCM Candidates:
Nursing staff:
The ICU is staffed in a nurse to patient ratio of 1:1. All these ICUnurses are given introductory training in critical care nursing and undergo regular teaching programs conducted or arranged by the Deptt. of Critical Care &Emergency Medicine, to promote critical nursing care skills and knowledge throughout their stay in the ICU.
Medical / Surgical ICU Technicians:
Medical / Surgical ICU Secretary:
Medical Data Operators:
ICU Counselor:
Academic & Research
Instt. of Critical Care Medicine has a basic introductory as well a very detailed academic program for the rotating residents of other departments and its own residents and fellows respectively. The program includes lectures, symposium, journal club, case discussion, adverse event outcome discussions, audit, equipment training and bedside teaching.
The doctors in training in the department are individually taught the techniques of difficult airway management, optimal mechanical ventlation, weaning from mechanical ventilation, noninvasive techniques of mechanical ventilatory support and central venous and arterial line placements. The training related to intubations, central line placements are taught to them initially in a dummy so that they can practice repeatedly. We have a computer simulator for Arrhythmia detection and management for teaching purposes. They are also taught the philosophy of modern intensive care practice, the attitude of "DONOHARM" in intensive care management, the importance of refined diagnosis in critically ill patients to achieve successful outcomes and the advantage of using noninvasive monitoring and measurements wherever possible.
This department presents some of the best award-winning clinical research papers at National Conference of Instt. of Critical Care Medicine &Pulmonology.
DNB (Post Doctorate Fellowship) in Instt. of Critical Care Medicine
Critical Care and Emergency Medicine Department holds a two-year post-doctorate DNB course in Instt. of Critical Care Medicine. Theree candiates are taken every year. The candidate rotates through all the intensive care units and faculty drawn from the Department of Critical Care and Emergency Medicine Department, Pulmonology, Internal Medicine, Surgery, Nephrology, Paediatrics, Cardiology, Gastroenterology, Neurology and Neurosurgery conducts a well structured teaching program for him.
IDCC &IFCC (Fellowship in Critical Care under ISCCM)
Instt. of Critical Care Medicine conducts:
Critical Care Training Course for Nurses
Instt. of Critical Care Medicine is conducting a 6 months long modular training Course for critical care nurses. Each module consists of a day long programme with didactic lectures & hands on teaching at various skills stations.
This porgramme follow a modular format in which there is a contact day for one day every month. In each module, there are didactic lectures, interactive sessions and workshops for various topics of importance in day-to-day management of critically ill patients.
After each module, the nurses are given a project to complete during the intervening period. Assessment (MCQ based) is done in the last module and two candidates are awarded certification for their excellent performance. Besides the Main ICU nurses from other Critical Care areas as well as from other Hospitals of Delhi have participated and benefited by the course.
Advanced Cardiac Life Support (ACLS) Provider Course
Sir Ganga Ram Hospital (SGRH) is a certified center by American Heart Association (AHA) for conducting Basic Life Support (BLS) Provider Course and Advanced Cardiac Life Support (ACLS) Provider Course. The team of AHA certified ACLS instructors from SGRH ICU have successfully conducted 44 ACLS course both in the hospital (held quarterly) and in various hospitals outside Delhi. Courses have been held along various national critical care conferences.
Library & Teaching aids
Instt. of Critical Care Medicine has a dedicated library situated in the doctor’s lounge, which contains all major books, journals related to critical care, SCCM publications, guidelines, monographs and audiovisual material in the form of videocassettes, CD-ROMs. The department has 4 dedicated computers with printing facility and Internet with round the clock access to database like MDConsult. The hospital subscribes to most of the major international journals available online. Instt. of Critical Care Medicine Department has developed its own data management software, which is used in the Medical/ Surgical ICU and has its own projection facilities in the form of OHP and Multimedia. A hand on training on mannequins/simulators is provided by the department to the residents and nursing staff.
Major Publications & Presentations:
Articles:
Chapters:
Books Authored:
Paper presentation/Poster Presentation/Oral presentation/Abstract:
Chapters:
Journal Scan:
Dr. Prakash Shastri- Yearbook of Anesthesiology-5, Editors- Sehgal R, Trikha A, Jaypee, 2016;299-302
Paper presentation/Poster Presentation/Oral presentation/Abstract:
Chapters:
Journal Scan:
Incidence of and risk factors for severe cardiovascular collapse after endotracheal intubation in the ICU: A multicenter observational study. Perbet S, De Jong A, Delmas J, Futier E, Pereira B, Jaber S, Constantin JM. Crit Care. 2015;19:257.
Dr. Prakash Shastri- Yearbook of Anesthesiology-5, Jaypee, Editors-Dr. Raminder Sehgal, Dr. Anjan Trikha, Pg 318-320
Abstract:
Articles:
Abstract:
CME Articles:
Insulin Infusion Protocol (Human Insulin/Insugen). Ray S. Current Medicine Research and Practice. 2014;4(4):186–187. http://dx.doi.org/10.1016/j.cmrp.2014.08.007.
Case Reports:
Chapters:
Articles:
Abstracts:
Chapters:
Trauma The current scenario and need for relook at strategies to prevent mortality and morbidity. Dr. Prakash Shastri. Updates on Anaesthesia CME 2013. Pg 40-44
Approach to managing a febrile patient in intensive care unit. Dr. Prakash Shastri. ECAB Clinical Update. Pg 3-20
Forthcoming Events and Conferences (Events Calendar):
Downloads:
1. What is meant by Intensive Care Units (ICU)?
Intensive care units (ICU), also called critical care or intensive therapy departments, are sections within a hospital that look after patients whose conditions are life-threatening and need constant, close monitoring and support from equipment and medication to keep normal body functions going..
2. How can I admit my patient in Sir Ganga Ram Hospital ICU?
For admission in Sir Ganga Ram Hospital ICU, you can directly contact the consultant on duty in the ICU either through Sir Ganga Ram Hospital extension number (2090) or ICU Consultant number (9811370004). Consultant of your choice can also make bookings for bed in ICU.
3. What are different training programmes conducted by the department?
The department is presently conducting post-doctoral fellowship programme in critical care medicine for doctors. The centre is recognised by both ISCCM and National Board of Examinations. The department also allows Observership for doctors. There are also training programmes for critical care nurses and technicians.
4. How can I join as Sr. Resident in the department?
Any doctor with post-graduation (in Medicine, Anaesthesia, and Chest Medicine) or 5 years of post MBBS experience in critical care & emergency medicine may apply for Senior Residency. Selection is done after interview subject to availability of vacancy. Please contact the HR Department for information on vacant residency posts in ICU.
5. How can I apply for ISCCM/ DNB Fellowship programmes?
The department conducts interview from applicants for ISCCM Fellowship selection. For application, visit URL: http://www.sgrh.com/dept/criticare/critical.htm#Fellowshipform. For DNB Fellowship, the National Board of Examinations conducts entry level exam for selection and candidates are posted according to merit and choice basis. For detailed information, visit URL: www.natboard.nic.in.
Contact us:
Services:
Equipment
The Medical/ Surgical ICU is equipped with state of art equipment and cutting edge technology to provide basic and advanced life support, monitoring and drug administration etc. The list of equipment is exhaustive and includes the following types and makes-
A. Organ Support:
B. Monitoring:
C. Advanced Diagnostics:
D. Others:
Services
Procedures and Treatments:
High Frequency Oscillatory Ventilation (HFOV) -High frequency oscillatory ventilation (HFOV) is a type of mechanical ventilation used as a rescue therapy in patients with failure of conventional ventilation like severe ARDS or in patients with air leak syndromes like pneumothorax and pulmonary interstitial emphysema (PIE). Two HFOV ventilators (3100 B) were installed in 2011 and is frequently used in management of severe ARDS patients. Additionally, fellows are made familiar with the basics and mechanism of this mode.
Nitric Oxide Delivery System-NOxBOXmobile, Nitric oxide (NO) Delivery system was installed in 2011. This delivers NO gas into the patient breathing circuit with continuous monitoring of the gas concentration. Nitric Oxide selectively dilates blood vessels in only those lung segments that are actively participating in gas exchange (oxygen & carbon dioxide) at the alveolar-capillary level thus improves oxygen levels in the body.
ECMO: The department started offering ECMO as a treatment modality in suitable cases. 4 cases initiated in 2015 for indications airway obstruction due to malignancy, aluminium phosphide poisoning and ARDS.
Percutaneous Tracheostomy (PCT) -Our ICU was one of the first centers in India to perform Percutaneous Tracheostomy (PCT) in 2000. This is a minimally invasive procedure performed at the bedside done under bronchosopic guidance. More than 1500 PCTs have been performed and the same has been presented in many international and national conferences.
Cadaveric Donor Management Program-Sir Ganga Ram Hospital is one of very few centers in the country that has an established state-of-the art facility for transplantation for both, adults and children using cadaveric as well as from living donors. Under the program, a protocolised approach for management of the cadaveric donors is in place in the ICU.
Renal Replacement Therapy (RRT) -Round the clock, in house, Renal Replacement Therapy (RRT) is available in the ICU.
RRT facilities available include Intermittent Hemodialysis (IHD), Continuous Renal Replacement Therapy (CRRT) and Hybrid Therapy like Sustained Low Efficiency Dialysis (SLED).
Ultrasonography (USG)/ Echocardiography (ECHO) -Sonography has evolved to become one of the most versatile modalities for diagnosing and guiding treatment of critically ill patients. It consists of both cardiac (Echocardiography) and non-cardiac (lung, abdominal and vascular) ultrasound. The ability to assess hemodynamics and volume status non-invasively is immensely useful in the management of critically ill patients.
Point-of-care ultrasound applications such as lung ultrasound are gradually replacing traditional imaging modalities (i.e., chest X-rays), while the use of ultrasound for procedure guidance has been shown to reduce complications and thus to increase patients’ safety.
Sonography is also used in Focussed Assessment with sonography in trauma (FAST) in critically ill trauma patients to detect intra-abdominal injuries.
Bronchoscopy-Flexible Fiberoptic bronchoscopy has become an important diagnostic and therapeutic tool for the management of patients admitted in intensive care unit. Involvement of the respiratory system is common, whatever the underlying cause of disease that precipitates the critical illness. The safety and usefulness of bronchoscopy in well trained hands with appropriate precautions have led to its increasing use even in unstable and mechanically ventilated patients.
Patient retrieval:
Air Ambulance
This service was first started in 1992 by our ICU consultant Dr SC Sharma and till date more than 300 patients have been transported both nationally and internationally by air ambulance as well as in commercial flights. The air ambulances are fully equipped with life support systems, ventilators and monitors and a trained doctor and technician accompanies the patient during transportation.
Ground Ambulance
The ICU staff undertakes the patient retrieval services round the clock. For this the department has an intensive care/cardiac ambulance fitted with Multichannel Patient Monitor, Bird Avian transport ventilator, medical gases and vacuum, infusion pumps, defibrillator, pacemaker, all emergency drugs and instrumentation.
Emergency Services:
The hospital runs a fully equipped Emergency Unit runs round the clock.Annually, on an average 50000patients attend the emergency room. With a built up area of 4000 sq feet , the emergency unit has triage, consultation and examination areas, observation ward, minor OT, plaster and dressing rooms, ECG room, resuscitation room and doctors and staff rooms and patient waiting areas. There are13 patient beds cum trolley bay. All patient beds have piped gases, vacuum, Multichannel cardiac monitors from GE. The unit has infusion pumps, defibrillators, pace maker, ICU and transport ventilators, patient and fluid warmers and trauma management equipment. The emergency is also the nodal point of disaster management of the hospital. It is fully equipped to handle any type of emergency and resuscitation round the clock. Registrars from Medical/ Surgical ICU are posted in emergency by rotation. Consultants of Critical Care and Emergency Medicine Department are available 24 hours, seven days a week in the emergency.
The emergency unit is strategically located near the entrance of the hospital and next to the imaging department.
Keywords:
CASES:
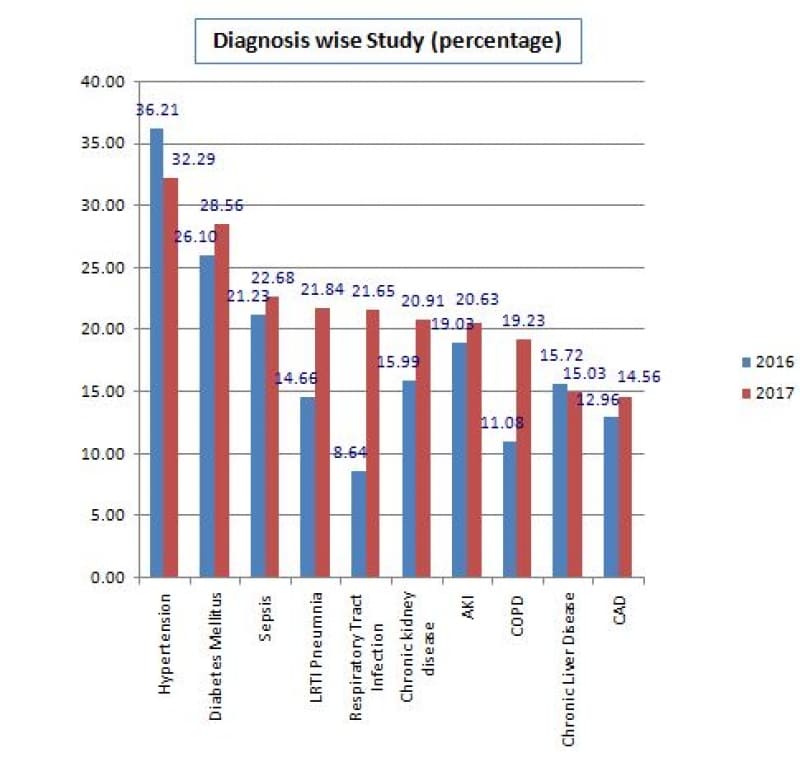
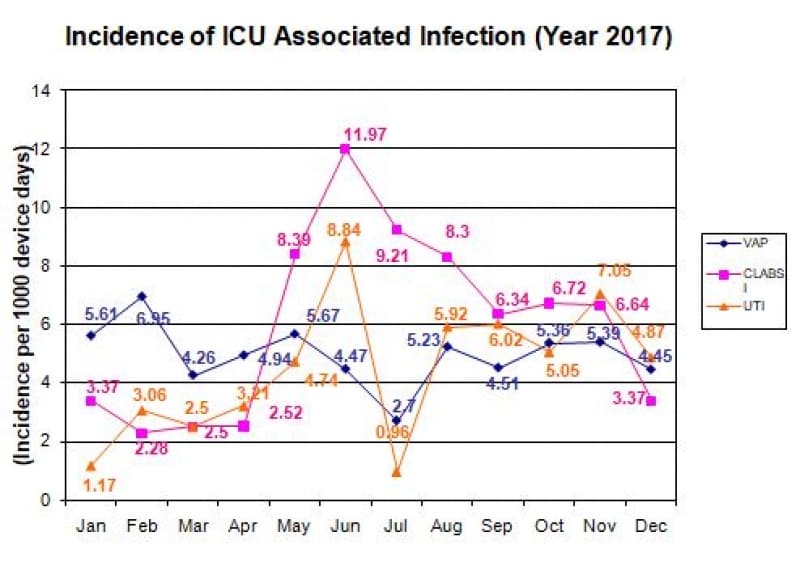
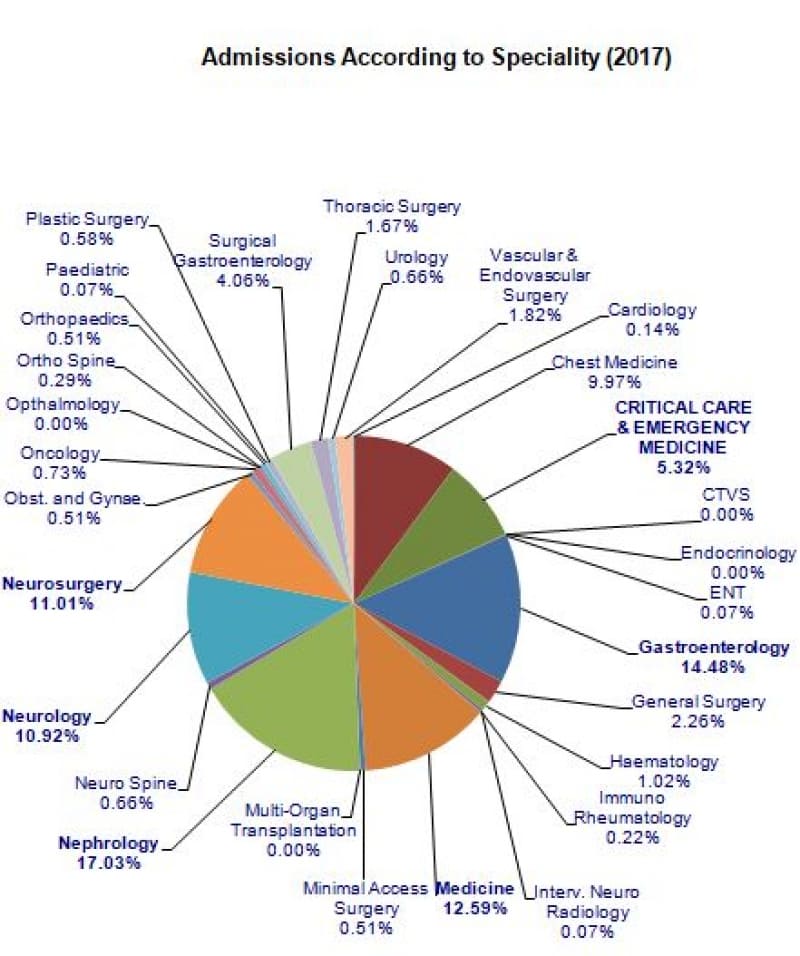
A total of 2143 patients were admitted in the ICU in 2017. Their admissions according to diagnosis and another chart showing incidence of ICU associated infection is as follows:
To correlate the APACHE-II scoring system with mortality and length of stay in ICU.
The Intensive Care Unit (ICU) of SGRH for the full year.
All adult patients who were admitted in the ICU were included. APACHE-II score was calculated with worst values of first 24 hours (at the completion of 24 hours). Patients who were discharged alive from the ICU or died after first 24 hours were noted as the primary outcome measurement. Patients who died or discharged within 24 hours were not included.

In the score category 11-20, 316 out of 386 patients (81.8%) were discharged and only 70 (19.2%) died. Out of those 780 patients whose APACHE-II score was found in high category 31 - 40, 56 (46.67%) deaths were observed.
On this parameter our ICU has been doing well for last 6 Years.
The APACHE-II scoring system was found useful for classifying patients according to their disease severity. There was an relationship between the high score and higher chances of mortality.
Correlation of APACHE II, Duration of Stay and Mortality

Majority of patients with APACHE < 20 survived. ALOS in survivors was much less than non-survivors. In case of severely sick patients, i.e. APACHE > 30; the observed mortality was much less than expected mortality.
Correlation of APACHE II, Age and Mortality

Except for APACHE > 40; the average age of was similar in survivors and non-survivors group.
Correlation of APACHE II, Age, Gender and Mortality

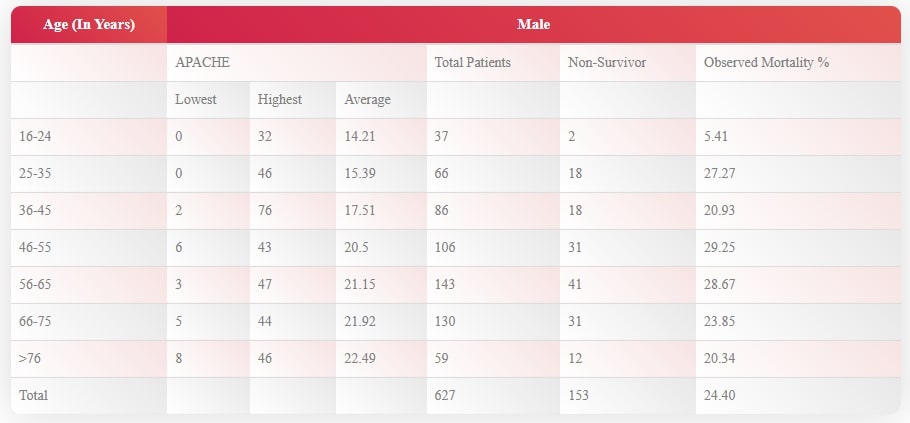
The number of male admissions is almost the double of the number of female admissions. The observed mortality is slightly higher in males (24.4%) as compared to females (20.55%); especially owing to the increased mortality in 25-55 age group.
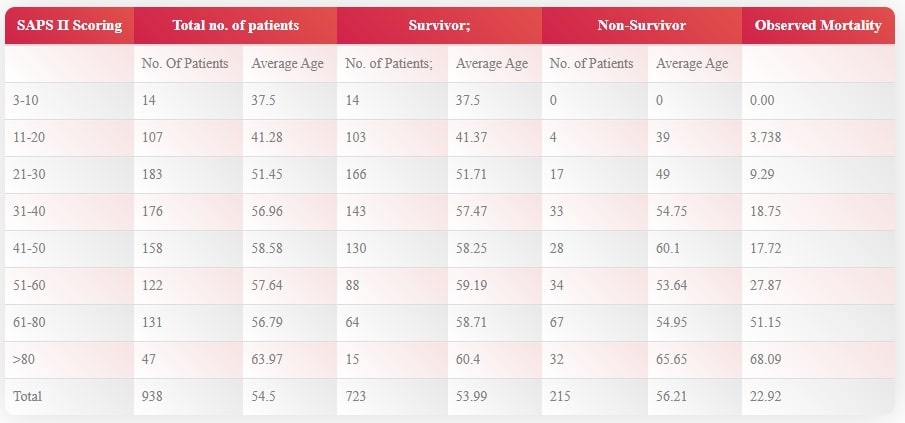
SAPS-II Score Correlation with Mortality
To correlate the SAPS-II score system with mortality in ICU.
The Intensive Care Unit (ICU) of SGRH for the full year.
All adult patients who were admitted in the ICU were included. SAPS-II score was calculated with worst values of first 24 hours (at the completion of 24 hours) Patients who were discharged alive from the ICU or died after first 24 hours were noted as the primary outcome measurement. Patients who died or discharged within 24 hours were not included.
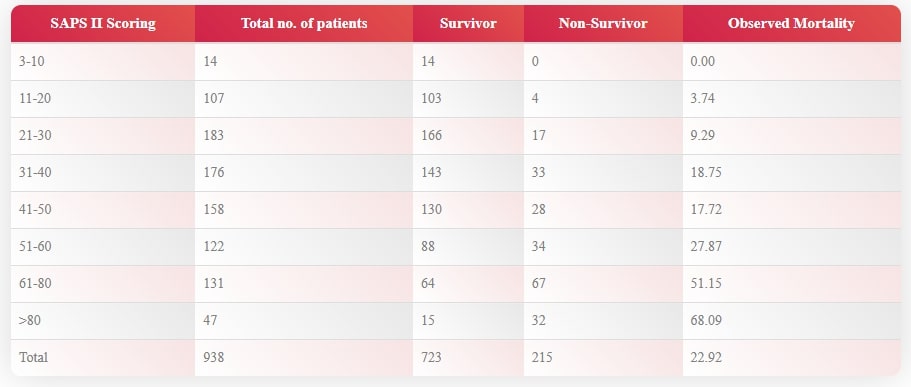
The SAPS-II scoring system was found useful for classifying patients according to their disease severity. There was a relationship between the high score and higher chances of mortality.
Correlation of SAPS II, Duration of Stay and Mortality

Correlation of SAPS II, Age and Mortality