Care of newborn babies has vastly improved in India over the last two decades and has seen major developments both in terms of improving strategies for newborn care in resource-poor societies and high-end technology-driven intensive care. The Department of Neonatology takes pride in undergoing this transformation. This unit came into existence in the 1970's. This was one of the first few level IIIB accredited units in northern India. With improving technological and medical expertise this unit has established itself as one of the best, not only in Delhi but also in India.
About the unit
We being one of the largest units have about 1200-1500 admissions per annum. This unit has 4 separate areas – consisting of two ICU’s (Intensive Care Unit) areas

and two step-down Intermediate care units (High dependency units)

Our NICU is a 37 bedded level unit, comprising of 16 ventilated beds each with wall-mounted new generation multi-parameter monitors equipped with the latest SET Masimo technology and inbuilt pulmonary graphics.The step-down areas can accommodate 21 babies; this area is similarly equipped with the multi-parameter monitor on each bed. Each monitor is further connected to a master screen monitor placed at the nursing stations wherein all parameters of the babies can be visualised on one large screen. All babies are nursed in the thermo-neutral environment under radiant warmer/incubator

Strength of our unit comes from the "State of the Art" Obstetrical and perinatal services rendered in the hospital, which attracts the large number of high-risk deliveries both from within Delhi and all over India. The NICU services are covered by 6 consultant neonatologist,

along with 10 post-doctoral resident doctors including DNB neonatology fellows, NNF ( National Neonatology Forum) fellows, and GRIPMER ( The Ganga Ram institute for post graduate medical education and Research) fellows. We were among the first intuitions to start the DNB & NNF fellowship programs. We have a nurse: baby ratio of 1:2 for the intensive care area and 1:3 ratio for babies not requiring intensive care. Apart from the newborn care area, our unit also offers a special lactation room where mothers are provided lactation counselling and can also express their milk with the help of multiple electric breast pumps.
The unit takes pride in providing state of art humane intensive care and this is reflected by our census which shows a survival rate for babies weighing < 1000 gms close to 70% which increases to 95% in babies weighing > 1000 gms. Similarly, the survival rates of babies more than 28 weeks is more than 95%. Our incidence of sepsis has drastically decreased to less than 2% due to better and evolving practices like - aggressive enteral nutrition, non-invasive ventilation and good quality initiatives. The above survival rates are comparable to the Western data.
The strength of excellent Neonatal care is provided by the nursing staff and they form the backbone of our unit and are an integral part of our rise to a state-of-the-art accredited unit providing optimal care to the tinest and sickest of babies. We are proud and blessed to have the support of 80 highly trained & experienced neonatal nursing staff who ensure round-the-clock quality care to our babies

. We cannot thank them enough for their services and their efficient nursing care forms an important cogwheel in our neonatal care and improved outcomes.
Services
Mechanical ventilation: Sick/preterm infants may have lung immaturity/dysfunction. These neonates may require ventilator support. The NICU takes pride in declaring that it was the first unit in private set up to start ventilation and today we handle the most difficult and tricky ventilatory strategies with great success.

High-Frequency Ventilators: Babies who have severe lung disease may fail on conventional ventilators. Our Unit has one of the best high-frequency ventilators for supporting such babies and were one of the first units to start using this technology.

Surfactant delivery: Premature lungs are deficient in a substance known as surfactant, leading to a stiff lung and breathing difficulty. In this situation, commercially available natural surfactant is instilled into the baby’s lung through a special tube. Giving surfactant to these babies improves their lung function, helps them to come off the ventilator faster, and ultimately help in improving survival and reducing lung injury. We have now started administering surfactant through non-invasive techniques like a laryngeal or supraglottic airway (SALSA) and this proves less traumatic on these small babies. We are presently conducting a randomised trial on the use of this non-invasive technique.
We are also one of the few centres to practice and utilise the technology of bedside lung ultrasound

to assess and decide therapy for babies with HMD ( Hyaline Membrane Disease).
Inhaled nitric oxide: Babies who have severe respiratory failure with high pulmonary artery pressure may require inhaled nitric oxide (a gas delivered into the lungs) to maintain adequate oxygen levels in blood. We are amongst the few units in India which has the experience of using nitric oxide and facilities for monitoring of such critically sick babies.

With the advent of this gas the outlook and outcome of babies with hypoxic respiratory failure has vastly improved.
Parental nutrition: Because of poor swallowing capability and immature gastrointestinal functions, the small preterm and sick baby is not able to tolerate oral feeds well and requires intravenous nutrition in the form of glucose, fats, and proteins for better survival. This parenteral nutrition is prepared by aseptic precautions under a laminar flow
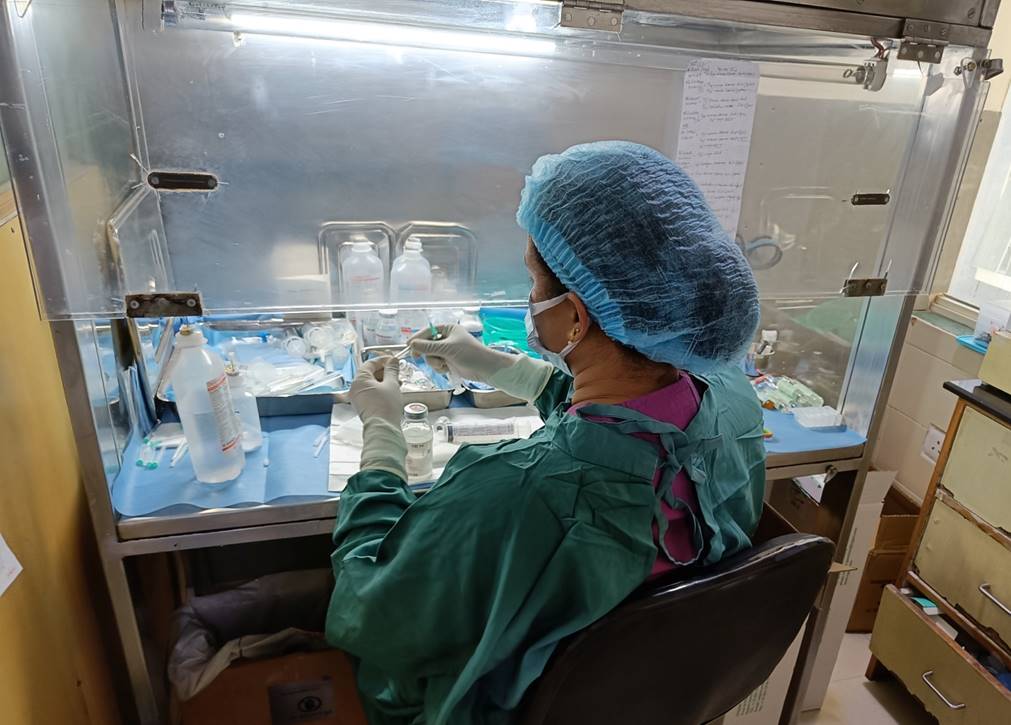
and is delivered via an intravenous route, till the time the baby is able to tolerate oral feeds. Not many units in India use laminar flow for aseptic preparation of Parenteral nutrition and drugs. This parenteral nutrition usually is given through central lines.
Intravascular lines: The advent of technological advancement and expertise in Neonatal care has lead to the survival of the tiniest, most premature, and sickest of babies. This has only been possible with skilled and expert central line insertion techniques.

We routinely perform both central venous access ( umbilical, PICC, and femoral) ) and central arterial access ( umbilical and peripheral) in all these babies. These intravascular lines has gone a long way in helping the survival of such babies as it helps in better nutrition, drug delivery, use of inotropes, blood pressure monitoring, and ease of sampling. Today we can also boast of advanced USG-guided central line insertion of the Internal Jugular vein.

Phototherapy and Exchange Transfusion: Babies who develop significant jaundice require special lights called phototherapy for their management. We have more than 10 such units including the latest technology LED ( Light Emitting Diode) phototherapy

and bili-blankets. Some Babies who don’t respond to intensive phototherapy may require exchange transfusion. We do around 10-15 such successful exchange transfusions per year. Most of these babies are extramural babies.
Bedside Echocardiography: Bedside echocardiography is a very important tool in the diagnosis and management of heart problems in premature as well as term babies. We are very fortunate to have such services available round the clock and this has made a big and significant difference in improving outcomes in such babies. All neonatal echo are done bedside by Neonatal cardiologists.

Neuroimaging: Premature babies are prone to have intraventricular hemorrhage (brain hemorrhage), especially in the first week of life. Very preterm infants are periodically evaluated with bedside ultrasound by sinologists,

who are available round the clock. Facilities of advanced imaging like MRI, Diffusion-weighted MRI, and MR Angiography are also available at our center.
In the case of bedside ultrasound showing enlarged ventricles ( sacs in the brain containing fluid) called hydrocephalus, we usually perform bedside ventricular taps to ascertain infections in the brain and ventricles. We are also proud to say that we perform state of art neonatal brain surgeries including the insertion of shunts both ventricular subgaleal and ventricular peritoneal.
Cerebral Function Monitoring: Sick babies are usually sluggish and neurologically depressed and need careful monitoring of their neurological status. We boast of one of the best bed side CFM ( cerebral function monitors) with video assistance technology which helps in the diagnosis and prognosis of these sick babies.
It also helps us in detecting subclinical seizures and thereby helps in their management. We also perform bedside EEG in babies with neonatal Encephalopathy

We now offer body cooling ( Therapeutic hypothermia) in the firt few hours of birth in a select group of babies who are born depressed and hypoxic at birth. This intervention has been shown to have improved outcomes in these babies.
Eye Examination: Retinopathy of prematurity (ROP) is a disease of very preterm babies, which can lead to blindness if not treated in time. To prevent ROP, a team of very experienced neonatal ophthalmologists,

periodically examine the retina of these preterm infants as per international guidelines. Babies with advanced stages of ROP are offered advanced ophthalmic interventions like bedside laser therapy and anti-VGEF drug instillation to halt the progression of disease and improve visual outcomes.
Universal Hearing screening: All babies born in hospital are subjected to an OAE (otoacoustic emission) test which is done to pick up babies with hearing loss.

It is a simple bedside test done in the hospital. Some babies may require advanced tests like Brain stem evoked response audiometry (BERA), which is also available in our hospital.
Genetic counseling services: All babies born or admitted to our hospital are universally screened for certain metabolic/ genetic diseases like hypothyroidism, G6PD deficiency, and congenital adrenal hyperplasia. For this, a few drops of blood are collected on a filter paper. Sick neonates with congenital anomalies or suspected inborn errors of metabolism are evaluated extensively with the help of geneticists. We are fortunate to have one of the country’s best and state of art genetic departments with an advanced testing centre and comprehensive counselling.
Lactational Support: We are proud to be able to have a dedicated lactation counselor who takes sessions on breast-feeding and helps mother with the expression of breast milk.

She is also actively involved in stimulating mothers to express their milk timely and explains the different techniques of expression and advantages of human milk. She also spends valuable time helping relieving & counselling parents of sick neonates in the NICU.
Developmental supportive Care: A team of Developmental Pediatricians and an Occupational therapist and support staff visits the nursery regularly and remains involved in the developmental support of the sick preterm babies. We try to give physical, visual, and auditory stimuli once sick babies are stable, for their faster recovery and rehabilitation. We are very sensitive with the noise and light levels in the nursery and this is continuously monitored with devices within the unit. We make our best effort to do “bundle of care” services to minimise pain and discomfort to our babies. Mothers are also involved in the care of the baby; they are encouraged to hold the baby next to their skin (Kangaroo Mother Care), which helps in better growth and development of infants apart from helping in establishing lactation.

Fetal medicine: Antenatal monitoring of the fetus for diagnosis and management is an essential area of Perinatology. We have the Department of Fetal Medicine where various antenatal procedures like amniocentesis, chorionic villous biopsy and intrauterine transfusion, etc are done, and appropriate counselling offered.
Allied Pediatric Sciences
Neonatal surgery facilities: We have excellent facilities for neonatal surgeries with 3 senior Pediatric Surgeons attached to the unit who are vastly experienced in surgical repair of anomalies such as congenital diaphragmatic hernia, trachea-esophageal fistula, intestinal atresias, imperforated anus, omphalocele to name a few. Even the tinest of babies are operated for some of the most complex anomalies and neonatal surgical conditions with good outcomes.
Neonatal Cardiac Sciences: A team of Pediatric cardiology and cardiac surgeons help us manage babies with complicated heart disease that occur at or after birth.

Our Cardiac Surgeon holds immense experience in operating cases such as Transposition of Great Arteries/Tetralogy of Fallot/Complex Congenital Heart disease. Functional Echo and bedside PDA ligations are routinely done in our NICU by the cardiac team.
We are among one of the few units in the country who perform advanced cardiac surgeries and have the backup of ECMO ( Extracorporeal Membrane Oxygenation) which is a life saving modality in severe lung disease and post-cardiac surgery babies.

Others: Sir Ganga Ram Hospital is one of the largest super-specialty hospitals of the country. As such we are fortunate to have Pediatric neurosurgery, Pediatric Nephrology, Pediatric Neurology, Pediatric Endocrinology, Pediatric haematology & Oncology, and Pediatric Gastroenterology-all under one roof. We do seek the help of these specialties if required. With their great expertise and clinical judgement we are amongst a few of the centres who provide for a gamut of specialised procedures like PEG ( Percutaneous Endoscopic Gastrostomy) tube insertion, bedside bronchoscopies, bedside tracheostomies, bedside dialysis,

ventriculo subgaealal (VSG) shunts to name a few.
iNICU: We are now in the process of going paperless with the advent of artificial intelligence with computer-based integrated neonatal care. This step puts us in the forefront of advanced neonatal care with high-grade quality initiative. This would go a long way in channelizing our data collection and analysis for future research projects and publications.
Neonatal Transport Services
Transporting sick newborn babies in our country is a major challenge. Our unit has two transport incubators with inbuilt ventilators with the help of which even very sick babies can now be safely transported.

We offer transport services round the clock. In the last 20 years, we have transported more than 1000 babies by road including 28 air transports. We have airlifted babies from all parts of India and a few even from neighboring countries.

We have a 24x7 helpline no-9599335877 to deal with all transport-related queries.
Academic Programme
The unit is the first in the country to be accredited with DNB neonatology program (Post MD Neonatology training) equivalent to DM Neonatology in the year 2005. Our pass percentage in the last 18 years of our DNB program is more than 95% and we always attracted the first two candidates selected in the common entrance test. Our students have won the Best DNB fellow award multiple times. We also have a very successful NNF fellowship program and were the first unit to start such a fellowship program. We now have collaboration with other institutions in the country conducting DNB and DM programs and do exchange program and sharing data for better learning skill of our postgraduates.
Quality care initiatives
It is very important to have inbuilt quality care initiatives in the management of patients and we are doing number of initiatives like Hospital care-associated infections audit, hand washing procedure audit, Insertion and maintenance bundles for the central lines, Surveillance information sheet, ventilator-associated infection audit and human milk audit for preterm babies. The plan for the future years is to compare the various audits of our department with other departments in the country and outside and use this data to further improve our neonatal care to further boost our survivals.
Research, publications, and Awards
The department has been involved in a number of National (Public Health Foundation of India ) and International researches (National Institutes of Health). We take pride that there have been a number of research publications in indexed renowned National & International journals from our unit. Our Departmental research paper has won NNF gold paper award a number of times in our National Neonatal conferences. Understanding the need for strong methodological evidence based clinical practice today, our unit pushes forward research activities by our neonatal fellows and at one given time, 8 – 10 research projects are ongoing. We look forward to keep research and publications one of our top agenda and put Sir Ganga Ram Hospital on the international neonatal research map.
Organization activities & Positional helds: Our department is very active academically holding National and International conferences and CMEs. The recent past saw two big international conferences “International Conference of Neonatal Nursing (2008)” and “Federation of Asia Oceania Perinatal Societies annual congress 2010” which were organised and successfully conducted by the departmental faculty members. The faculty members are all involved in National Neonatal skill-based training for Tier 2 & 3 centres in the country to improve skill of Neonatal providers thereby improving neonatal care to all. All faculty members are accredited trainers for National Resuscitation Programme ( NRP) and are actively involved in training and conducting of these workshops. We have been doing yearly departmental CME & Workshops in the months of February/ March regularly for the last 20 years.

It is one of the CME which is much awaited by delegates all over the country and is always appreciated for its academic feast and evidence-based bed side teaching. We usually discuss important and relevant topics like Neonatal Nutrition, Basic & advanced ventilation, Bedside procedures, Recent advances in Neonatology, Functional Echo and point of care ultrasound, Statistical Methodology, and analysis.
Our departmental faculty members have also held multiple important International and National professional bodies posts and positions to be proud of. Some salient ones that make us stand out are - Secretary FAOPS, President and Secretary National NNF, President, Secretary, Joint Secretary and member Delhi NNF, Secretary & President Elect Delhi IAP, Editor in chief and member editorial board CMRP journal, Course coordinator PCNI.
Audit
The department has been collecting data of all neonates and a perinatal audit is carried out ever year by the department which is also published in the annual hospital audit committee publications. We were part of the National Neonatal Perinatal Database also in year 2000. We are now also part of national and international collaborations and have started sharing data with each other so as to further improve neonatal care and outcomes in our hospital.
“Everyone needs the world and the world needs everyone”. The department cannot work in the illusion of solitude but rather exists in its persuit for excellence with immense support from the institute, parents, nurses and society at large. We strive to bring smiles on our babies faces and happiness and joy to their parents.